

Oral Fluid Testing
Examining issues and limitations with the technology
Counterpoint Volume 8: Issue 1 - Article 2 (March 2024)
An article in the upcoming Mastery Skills I-4 Module
Jan Semenoff, BA, EMA
Forensic Criminalist

|

|
Article information:Article - 2300 words (approximately 12-15 minutes)
Video - 25:43 |
The video
In the same way that police officers rely upon Approved Screening Devices (ASDs) or Preliminary Breath Test devices (PBTs) to screen for the presence of alcohol, new technologies are now being deployed to detect recent use of recreational drugs, drugs of abuse, and illicit substances. Enter Oral Fluid Testing (OFT), where a sample of saliva can be analyzed to detect several classes of compounds (as opposed to specific drugs).
Let’s look at this technology, and the advantages and disadvantages it presents.
Let’s look at this technology, and the advantages and disadvantages it presents.
Saliva
First, we should look at the characteristics of the substance being used as a test medium – saliva.

|
Understanding blood, breath, and urine samples seems relatively straightforward. Saliva, on the other hand, is actually quite a complex fluid, with more in there than meets the eye. Saliva is an extracellular fluid produced and secreted by the salivary glands in your mouth and oral pathway. Don’t let the term “extracellular fluid” add any confusion. That simply means that it is a body fluid found outside the cells of a multicellular organism. In other words, the salivary gland cells secrete the saliva outside, into the mouth and oral pathway.
|
Human saliva is about 99.5 % water, with the remaining components consisting of:
- Mucous – A slippery liquid produced by the secretion of the mucous membranes. It sounds gross, but you need that mucous to protect the linings of your respiratory and digestive systems from spicy foods, fatty or fried foods, or corrosive beverages such as alcohol or coffee.
- Electrolytes – Sodium, potassium, calcium, magnesium, etc.
- Epithelial (skin) cells,
- White blood cells,
- Digestive enzymes used to break down starches and protect the stomach wall lining, and
- Antimicrobial enzymes to kill bacteria.
The DNA of a person tested can be extracted from the epithelial cells and is commonly tested in commercial DNA kits from companies like Ancestry or 23andMe. Human saliva contains as many as 8 million human and 500 million bacterial cells per mL. Yuck! |
The enzymes found in saliva are essential in the digestive process, breaking down dietary starches. When your parents told you to chew your food slowly, it was so that the enzymatic action made it easier to break down your food.
For our purposes, we are concerned with saliva as a chemical solvent, treating it like the liquid medium it is that carries dissolved solutes (or substances). Because there is so much bodily fluid or water in saliva, it will rapidly become saturated with any substance that dissolves or can be suspended in bodily fluid, like alcohol or drugs.
How long do drugs stay in your saliva?
Here is a rough guide for detection times in humans. It is an estimate only, as detection times can vary depending upon the strength of the drug taken, its dose, the person’s size or weight, the person’s tolerance to the drug, and if it was mixed with other substances that could alter the metabolic clearance rate of the substance. So, consider as a very rough guide the comparative retention times of various drugs in saliva, versus blood or urine:
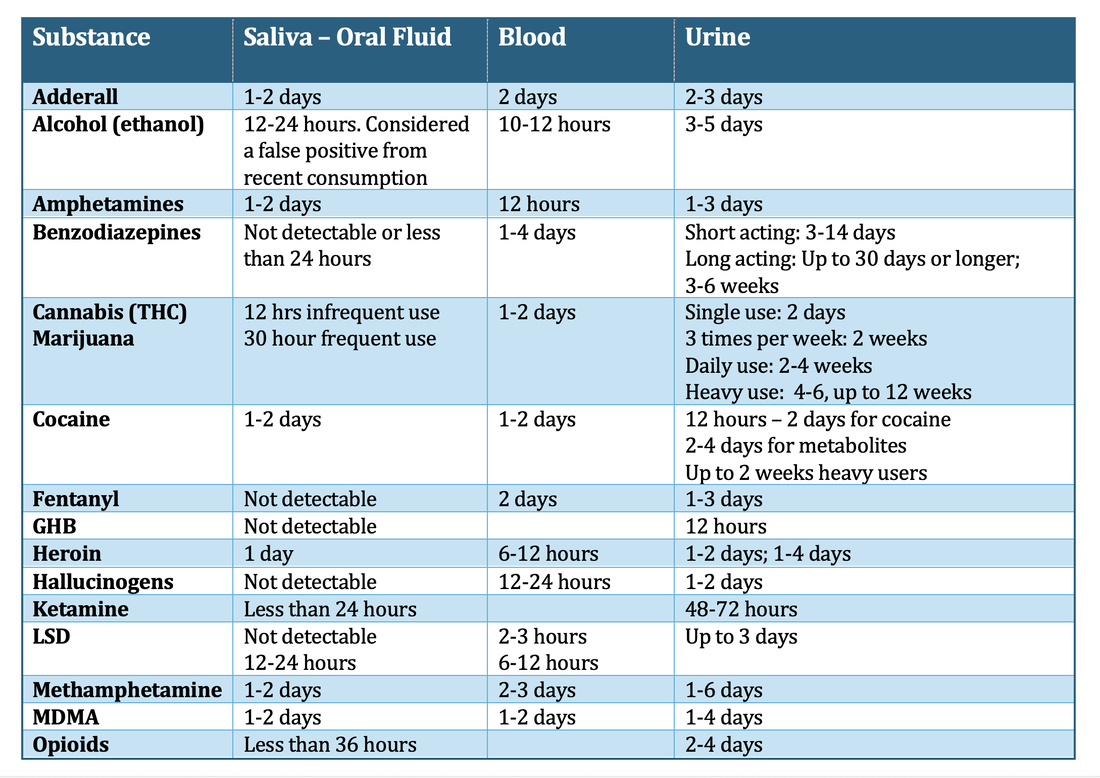
Table 1 - Retention times of various drugs as found in saliva, blood, or urine. These are ROUGH ESTIMATES ONLY.
|
Click here to download the table in .pdf format for your reference library
| |||
In general, we can say that OFT has a typical detection period of less than 48 hours, with urine testing a range of up to four days for most drugs, and up to 30 or so days for cannabis. Since most substances can’t be detected in saliva for longer than two days, testing within the appropriate window of time is crucial for accurate results. For this reason, saliva drug tests are often used to identify current or recent drug use, and as a result, may not be ideal for testing chronic drug users.
Note: I was going to add a column to show the drug retention times for Hair Segmentation or Hair Follicle testing, but they are ALL about 90-180 days.
Oral fluid testing technology
It’s important to recognize that some drugs, such as cannabis based compounds, can remain in the urine for weeks after use, and may take some time before being acquired in the urine. It is generally considered that Oral Fluid Testing can usually detect recent drug use within 30 minutes to 48 hours after use. See below for our examination of this claim.
Also, OFT is limited to detecting a class of compounds, or their parent compounds, rather than distinguishing a specific drug. The distinction is important. As an example, OFT might flag a sample for Cannabis (THC) and is unable to distinguish the positive result from Marijuana, Hashish, or Cannabidiol (CBD Oil).
Some manufacturer’s use undiluted oral fluid, often referred to as “neat fluid”, in the collection and analysis process. Other manufacturers will collect the oral fluid on an absorbent pad, and then introduce this neat fluid to a buffered solution which dilutes it prior to analysis. The advantage of the diluted solution is that it can preserve it, preventing bacterial growth, so that it can be transported at room temperatures and further analyzed. It also makes it easier for the sample to move across the test medium, as we will see.
Types of substances that can be detected by OFT:
- Alcohol
- Amphetamines
- Barbiturates
- Benzodiazepines
- Cocaine
- Marijuana
- Methamphetamine
- Opioids
- Opiates
- Phencyclidine
Immunoassay testing
Urinalysis using immunoassay technology. This sample just tested positive for cocaine after the test subject had consumed a herbal tea made from coca leaves.
|
OFT uses a longstanding process called Immunoassay Testing. The Immunoassay (or IA) drug test uses antibodies to detect the presence of selected drugs and/or their metabolites based on a predetermined cutoff threshold. They have been commonly used in urinalysis, and now are employed in OFT.
They are qualitative (presence detected only) not quantitative (amount detected) tests and have been long identified as susceptible to producing both false-positive and false-negative results. Due to this limitation, they can only be used as screening tests.
|
The moment before I said the "F" word...
|
You're probably already familiar with Immunoassay Testing technology...
If you’ve ever provided a urine sample at the doctor’s office to check your blood glucose levels, or used a home pregnancy test to see if you are pregnant, you’ve had an IA test. If you’ve ever stuck a swab up your nose to test for COVID-19, you’ve performed an IA test on yourself. When you stuck the swab (containing the neat fluid from your nose and sinus cavity) into the fluid vial of the test kit, it was the buffered solution that analyzed the diluted nasal or oral mucous sample. Ya, I know… like we ever want to go through that again! |

|
You will recall the one consistent factor in this testing methodology – a line was formed, or a color change occurred to the test strip, based on it surpassing the levels predetermined as the cutoff threshold. It is as simple as that. Positive line on the test strip, and you’re pregnant, or have COVID. The orange box changes to green on your urinalysis, and your blood glucose is over a threshold amount.
|
But it is that same technology – the color change in a chemical test strip, that is used in the latest electronic drug screening devices.
Units such as the Dräger DrugTest™ 5000, which we will discuss below, simply read this color change on the test strip with an optical reader. Nothing more. What’s more – it’s a qualitative change that is read. The result is either positive or negative with no attempt made to quantify the results (regardless of what the test technician testifies to).
Advantages of oral fluid testing
In the US, there are mandatory guidelines for Federal Workplace Drug Testing Programs. As a result, many drug tests are performed either as random, pre-employment, or post incident tests every day in workplaces across North America.
Here I am providing an oral fluid sample.
And, yes... it sucked!
|
OFT is quick, non-invasive, and painless. It offers a low cost-per-use sampling, with test results available in minutes. It can detect recent drug use, but not historic drug use.
In comparison, blood analysis is invasive, can be painful, is expensive and has turnaround times measured in days or weeks.
But again, since it is only a screening result, it must be followed up with a quantitative test for any positive results to be considered reliable. Basically, its strength is in screening out negative results quickly and cheaply.
|
Disadvantages of oral fluid testing
Drugs and drug metabolites do not remain in oral fluids as long as they do in urine, and as a result the detection window is two days or less.
Quantification
Because of this two day “window”, OFT cannot distinguish between a large dose of a substance taken 48 hours ago versus a small dose taken 30 minutes ago. The results will simply generate a positive reading that must be empirically verified in another way, typically by a blood draw. Urinalysis is also unable to distinguish a quantitative level at a point in time.
Also, unlike breath alcohol testing, where a legislated blood to breath ratio (such as 2100:1 in North America, or 2300:1 in the UK) establishes a correlation between the breath sample BrAC and the blood sample BAC, there is no conversion factor available in OFT. There is no correlation between the amount of THC in the saliva versus the amount of THC in the blood, as an example.
There are currently no reliable instant saliva testing products that have FDA approval that also test to approved cut-off levels. OFT has not been able to test with 100% accuracy at concentrations 25% below or above the cut-off levels for the immunoassay used.
As a result, OFT can only be used as qualitative screening devices, and can never create a quantitative reading. Both false negative and false positive results are well documented and reported in the scientific literature regarding OFT.
False positives
In general, OFT is less accurate than blood or urine testing. False positives are possible from recently consumed foods, gums, tobacco, or other products and require an observation and deprivation period like those performed for breath alcohol testing.
Here, a test subject who has never consumed a cannabis substance in their life tested positive for THC after using a drop of this CBD oil 30 minutes earlier.
|
Immunochemical or immunoassay detection reactions are NOT specific to a single drug (in chemistry or pharmacology, called an analyte), but rather, reacts to a group of drugs (analytes) with similar chemical structures.
Since they do not identify a specific drug, only its class of drug, they can and do provide false positive readings, as discussed below with the Dräger DrugTest™ 5000. Specificity is an issue with OFT. An innocuous (and legal) substance, like a poppy seed, may be mistaken for opioid consumption.
|
False Negatives
OFT can detect recent drug use, but not historic drug use. Cut-off levels, as previously discussed, cannot be considered due to the limitations of the technology. This can lead to a situation where the substance is actually in the OFT, but at a level below the cut-off level, and therefore will NOT be reported.
Accuracy, resolution, and qualitative analysis
Click the article cover to go to the article.
|
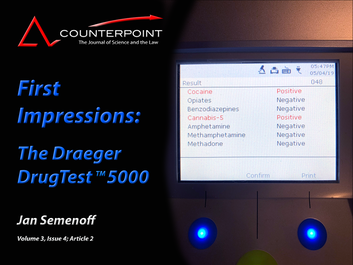
At this point I will refer you to the Counterpoint article, “First Impressions: The Dräger DrugTest® 5000”
(Counterpoint Volume 3, Issue 4 – Article 2) for an examination of one OFT device. Access online requires a subscription to Volume 3. Click here to download the free article in .pdf format for your reference library
| ||
That article describes our experimental design with the Dräger DrugTest® 5000 device. In short, we blind tested the device’s operator (me) so that I did not know who had used a cannabis product within 30 minutes of testing, and who was a control subject. I did not know who was a chronic cannabis user, or an occasional one.
We also did pre-use and post-test DRE evaluations. Our data indicated that there was no statistical difference in DRE evaluations in either group, or between users and control group participants. We concluded that DRE evaluations cannot detect recent THC usage.
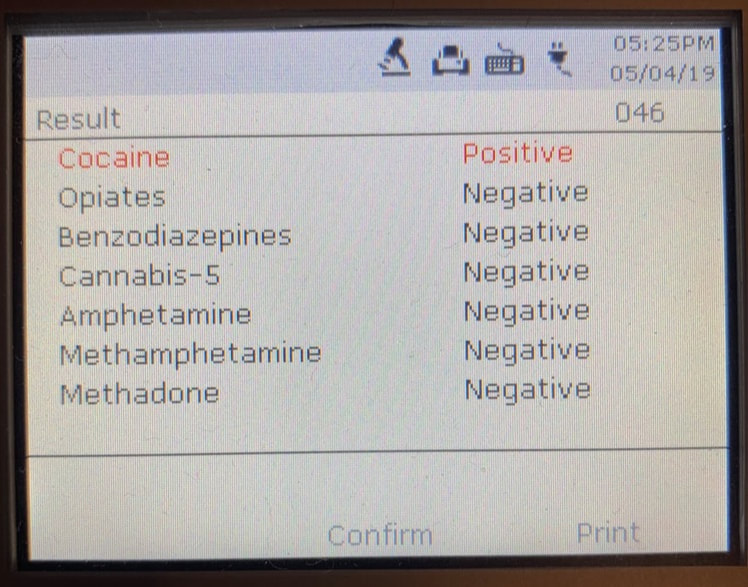
This is the OFT result from the same drinker of herbal coca leaf tea.
|
We also added a variety of false-positive producing substances into the testing equation to see if the device could identify potential contaminates.
We identified a series of failures of the Dräger DrugTest® 5000. We had positive readings from non THC users, negative readings from chronic or recent THC users, and positive hits for cocaine and opiates when herbal tea or poppy seed muffins were consumed.
Cannabidiol (CBD) oil produced a false-positive THC reading in a non-user of cannabis products. The incidents of false negative and false positive readings were about the same – 25% of reported results in either group were wrong.
|
Dräger is clear in the instruction for the STK that the results obtained must be confirmed by professional analytical assessment, preferably by GC/MS (Gas Chromatography/Mass Spectrometry) or LC/MS (Liquid Chromatography/Mass Spectrometry). Remember, Dräger has identified the inherent limitations of the technology used and, as such, views the DrugTest™ 5000 Analyzer as a “qualitative screening device”. End-users of the DrugTest® 5000 must keep that limitation in mind.
Regardless of the device used for testing, there is an overall concern as to the accuracy of OFT for THC. From Robertson et al, 2022:
|
There is a good correlation between the presence of THC in oral fluid and the presence of THC in blood. When using oral fluid THC as a biomarker for the presence of THC in blood, the sensitivity is 71.2% and the specificity is 97.7%. However oral fluid THC, at commonly used cut-off values, is less sensitive and less specific when used as a biomarker for detecting people with higher THC concentrations in blood. In particular, the positive predictive value of a positive oral fluid test, when used in to screen randomly selected drivers for “illegal” THC concentrations appears to be unacceptably low in jurisdictions with non-zero per se limits for THC in blood.
|
Final thoughts:
The limitations are clear. OFT technology is suitable only as a preliminary screening device and is known to provide readings with both false negative and false positive determinations. Any results generated, and any sanctions that arise from those readings, must be confirmed by a professional analytical assessment, and should not form the basis of job action or criminal charges.

Send me your questions or comments:
Comments and questions will be posted here with their responses:
Comments and questions will be posted here with their responses:
For further study:
- https://www.thermofisher.com/ca/en/home/clinical/diagnostic-testing/clinical-chemistry-drug-toxicology-testing/drugs-abuse-testing/drug-testing-overview/oral-saliva-drug-test.html#:~:text=Oral%20fluids%20detect%20recent%20drug%20use%20generally%20within%2048%20hours,urine%20for%20weeks%20after%20use.&text=Oral%20fluids%20generally%20detect%20parent,similar%20to%20circulating%20blood%20levels.
- https://www.govinfo.gov/content/pkg/FR-2015-05-15/pdf/2015-11523.pdf
- https://cdn.adf.org.au/media/documents/How_long_does_a_drug_stay_in_your_system_-_infographic_1.pdf
- https://www.goodhire.com/resources/articles/saliva-drug-test/
- https://www.aafp.org/pubs/afp/issues/2019/0101/p33.html
- Verstraete AG. Detection times of drugs of abuse in blood, urine, and oral fluid. Ther Drug Monit. 2004 Apr;26(2):200-5. doi: 10.1097/00007691-200404000-00020. PMID: 15228165. Found at: https://pubmed.ncbi.nlm.nih.gov/15228165/
- M.B. Robertson, A. Li, Y. Yuan, A. Jiang, H. Gjerde, J.A. Staples, J.R. Brubacher, Correlation between oral fluid and blood THC concentration: A systematic review and discussion of policy implications, Accident Analysis & Prevention, Volume 173, 2022, 106694, ISSN 0001-4575, Found at https://doi.org/10.1016/j.aap.2022.106694
